Imagine waking up with a gut that feels like it's at war with itself. For millions of people, this isn't a bad dream but a daily reality. Whether it's a sudden, urgent trip to the bathroom or a deep, aching pain in the abdomen, the symptoms of Inflammatory Bowel Disease can be terrifying and confusing. The biggest frustration? Many of these symptoms overlap, making it hard to tell if you're dealing with Crohn's disease or ulcerative colitis.
While both conditions fall under the umbrella of autoimmune diseases-where your immune system mistakenly attacks your own healthy tissue-they aren't the same. One acts like a targeted strike on a specific area, while the other is more like a random series of explosions across your entire digestive tract. Knowing the difference isn't just for doctors; it's the key to getting the right treatment and avoiding permanent damage to your gut.
Quick Summary: The Main Differences
- Location: Ulcerative colitis stays in the colon and rectum; Crohn's can hit anywhere from the mouth to the anus.
- Pattern: UC is a continuous stretch of inflammation; Crohn's often has "skip lesions" (patches of healthy tissue).
- Depth: UC affects only the inner lining (mucosa); Crohn's can penetrate through the entire wall of the bowel.
- Cure: Surgery can potentially cure UC by removing the colon; surgery for Crohn's manages symptoms but doesn't cure the disease.
Where exactly is the inflammation?
The easiest way to distinguish these two is to look at the map of the digestive system. Ulcerative colitis is a chronic inflammatory bowel disease that exclusively affects the colon (large intestine) and the rectum. It always starts at the rectum and crawls upward in a continuous, unbroken line. If you have UC, the inflammation won't suddenly jump to your small intestine or your stomach; it stays locked in the large bowel.
Now, Crohn's disease is a different beast. It's an inflammatory condition that can manifest anywhere from your mouth to your anus. While it loves the end of the small intestine (the terminal ileum), it doesn't follow a neat line. Instead, it creates what doctors call "skip lesions." You might have a foot of inflamed bowel, then a few inches of perfectly healthy tissue, then another patch of inflammation. This unpredictability is why Crohn's is often more complex to manage.
How deep does the damage go?
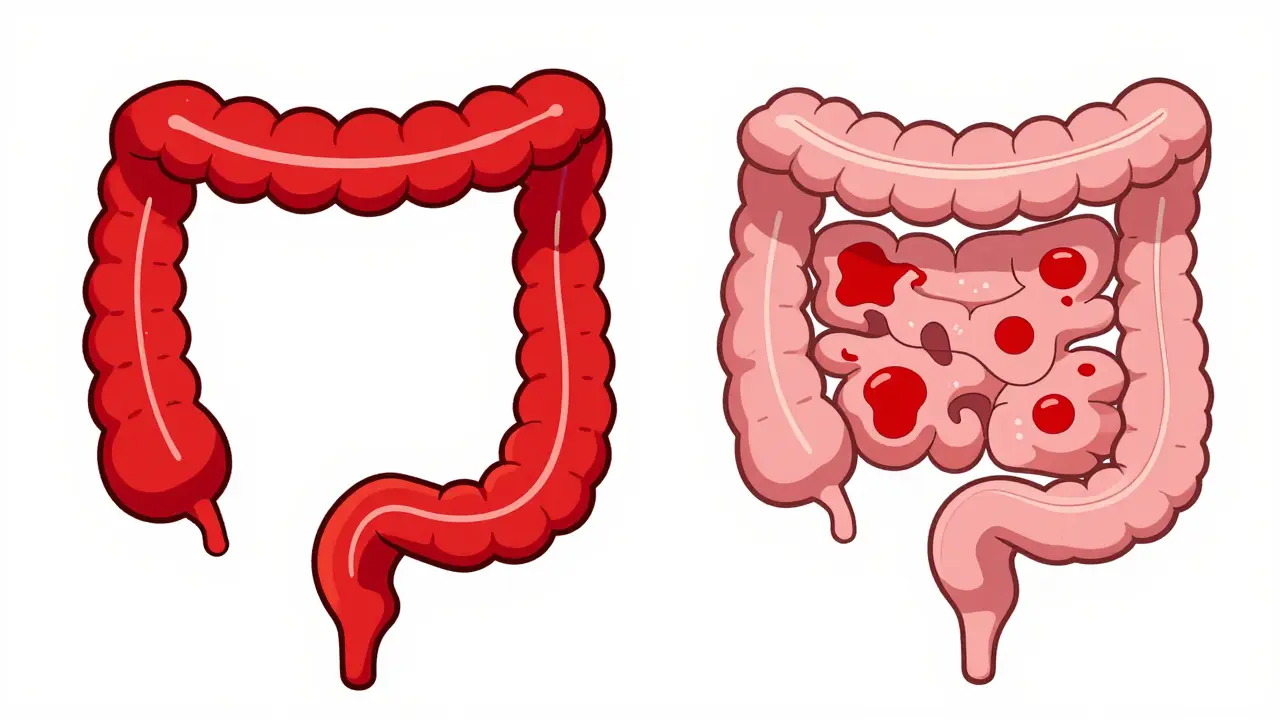
If we think of the bowel wall like a piece of plywood, ulcerative colitis only sands down the very top layer. It affects the Mucosa is the innermost lining of the gastrointestinal tract and the layer just beneath it. Because the inflammation is superficial, the primary issue is often bleeding and urgency.
Crohn's, however, is "transmural." This means the inflammation bores through every single layer of the bowel wall, from the lining all the way through the muscle and out to the outer skin of the organ. Because it goes so deep, Crohn's can cause the bowel wall to thicken and scar, leading to narrow passages called strictures. It can even create tunnels called fistulas, where the bowel accidentally connects to another organ or the skin of the abdomen.
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Location | Colon and Rectum only | Anywhere from mouth to anus |
| Inflammation Pattern | Continuous | Patchy (Skip Lesions) |
| Tissue Depth | Superficial (Mucosa) | Transmural (All layers) |
| Common Complications | Toxic Megacolon | Strictures and Fistulas |
| Surgical Outcome | Potential Cure | Management only (Not a cure) |
Spotting the signs: Symptoms and Triggers
On the surface, both diseases look similar: fatigue, weight loss, and abdominal pain. But if you look closer, the "flavor" of the symptoms changes. People with UC often deal with an intense sense of urgency-the "I need to go right now" feeling-and more frequent rectal bleeding. This is because the rectum is almost always involved in UC.
Crohn's patients often struggle more with nutrition. Since the small intestine is where most of our nutrients are absorbed, inflammation there can lead to malnutrition and significant weight loss. When it comes to triggers, the experience varies. Many UC patients find that stress is the primary spark for a flare-up. In contrast, those with Crohn's often report that specific foods-like dairy or high-fiber vegetables-trigger their symptoms.
The diagnostic journey: How doctors tell them apart
There is no single "magic test" that gives a yes or no answer. Instead, doctors use a puzzle-piece approach. The gold standard is the Colonoscopy is a medical procedure where a camera is used to examine the entire length of the colon . In UC, the doctor sees a smooth, continuous red inflammation starting from the bottom. In Crohn's, they see a "cobblestone" appearance-patches of swelling and ulcers separated by healthy-looking skin.
Blood and stool tests add more clues. A test for pANCA is an antibody found in the blood that is more common in ulcerative colitis . If this comes back positive, it leans the diagnosis toward UC. For Crohn's, imaging is more critical. An MRI or a capsule endoscopy (where you swallow a tiny camera) can find inflammation in the small intestine that a standard colonoscopy simply can't reach.
Treatment: Managing the fire
Since the diseases behave differently, the tools to fight them differ too. UC treatment often starts with 5-aminosalicylates (5-ASAs) are anti-inflammatory drugs used to treat the lining of the colon . Because UC is localized, doctors can use enemas or suppositories to deliver the medicine exactly where the fire is burning.
Crohn's requires a more systemic approach because the inflammation can be anywhere. Doctors often rely on Immunomodulators are medications that suppress the overactive immune system to reduce inflammation like azathioprine. Both diseases may use Biologics are advanced protein-based drugs that target specific parts of the immune system , such as anti-TNF agents, but they work differently depending on the disease's behavior.
The most striking difference is the role of surgery. If a person with UC has their entire colon and rectum removed, the disease is essentially gone because the target organ is gone. For someone with Crohn's, surgery is used to remove a damaged segment or fix a fistula, but the disease can simply pop up in a new spot nearby. It's a management tool, not a cure.

The ripple effect: Beyond the gut
These aren't just "stomach problems." Because the immune system is involved, the inflammation can spill over into other parts of the body. Many people with either condition experience joint pain or skin rashes like erythema nodosum. However, some connections are more specific. Primary Sclerosing Cholangitis is a rare liver disease where bile ducts become inflamed and scarred is much more common in those with ulcerative colitis than in those with Crohn's.
Can Crohn's disease turn into ulcerative colitis?
No, they are distinct conditions, but it is common for a patient to be misdiagnosed initially. About 10-15% of cases start as "indeterminate colitis," where the doctor can't tell which is which. Over time, as the disease progresses or complications like fistulas appear, the diagnosis is often updated from UC to Crohn's.
Which one is more severe?
Neither is universally "worse," but they present different risks. Crohn's is often more complex due to the risk of strictures and fistulas. UC can lead to life-threatening complications like toxic megacolon, where the colon expands rapidly and risks rupturing.
Do diet changes cure IBD?
Diet cannot cure IBD, but it can manage symptoms. While some Crohn's patients find relief by avoiding high-fiber foods or dairy during a flare, there is no single "IBD diet" that works for everyone. Medical treatment is necessary to achieve true remission.
Is IBD hereditary?
Yes, genetics play a significant role. If you have a close relative with Crohn's or UC, your risk is higher. However, the exact cause is likely a combination of genetic susceptibility and an environmental trigger, such as a change in the gut microbiome.
Can I live a normal life with IBD?
Absolutely. With the right combination of biologics, immunomodulators, and lifestyle adjustments, many people achieve long-term remission. The key is early diagnosis and consistent monitoring to prevent permanent scarring of the bowel.
Next Steps and Troubleshooting
If you're experiencing persistent diarrhea, blood in your stool, or unexplained weight loss, don't try to diagnose yourself using an online checklist. Your first step should be a visit to a gastroenterologist. Be prepared to keep a detailed food and symptom diary for two weeks; this data is incredibly valuable for your doctor to identify patterns.
If you've already been diagnosed and are struggling with a flare-up, check if your current medication is targeting the right "behavior" of your disease. For example, if you have Crohn's and are noticing a new, dull ache after eating, you might be developing a stricture. This requires a different management approach than a purely inflammatory flare. Don't wait for the pain to become unbearable-early imaging can prevent a surgical emergency.




Categories